Inpatient Psychiatry Resident Education in Quality Improvement (QI): A Guide to the 5th-floor
Authors : Patricia Guiribitey. MD, Adarsh Shetty. MD, Sruti Patel. MD, Gerardo Ferrer. MD
Abstract:
- Objective:
To increase the knowledge the new inpatient psychiatry residents, off-service residents, sub-interns, and medical students have upon starting inpatient rotation by which we can ease the transition of patient care.
- Methods
A 7-question survey questionnaire was developed by the research team to assess the knowledge gap and perceptions of the in-patient unit using the PDSA model. New off-service interns, sub-interns, and medical students were then given an orientation on the practices and protocols of the inpatient psychiatric unit. Another questionnaire followed this intervention to learn about their comfort level.
- Results
Respondents included around 30 medical professionals for a response rate of 70%. Over 65% of residents and students reported they will be rotating in an inpatient psychiatric unit for the first time, with ~35% rotating for the second time. Those who have rotated before in a psychiatric inpatient unit were significantly more confident than those who have not. Prior to the intervention, we asked residents about how to feel about starting the rotation, upon which the majority (39%) reported feeling calm/comfortable, with 11% feeling confident, and 6% feeling very confident. The rest (44%) felt either overwhelmed (11%), anxious (11%) confused (11%), and worried (11%). A strong culture for teaching was also considered important and was reported to be a vital part of the program.
- Conclusions
Overall, two-thirds of residents reported positive educational experiences with a strong sense of preparedness and low levels of anxiety. Continuing Inpatient Guide 101 improvements, including regular updates and keeping residents informed, is warranted. It will allow them to better use their time and be effective in their contributions as LCH residents/students.
- Keywords:
education, residents, psychiatry, training, students
Introduction
Larkin Community Hospital's south Miami campus consists of a 146-bed Acute Care hospital, it is a general medical, surgical, and psychiatric teaching hospital, located in South Miami, Florida. It is the sixth-largest statutory teaching hospital in Florida (by the number of postgraduate training programs) and the fourth largest (by specialties in supply/demand deficit in Florida)Larkin Community Hospital is composed of about 57.7% females and 58.3% ethnic minorities. The psychiatry unit at LCH south Miami campus is composed of 36 beds. The patient population is diverse, composed of Caucasian, African American, and Hispanic representation. The project started while doing our last inpatient psychiatry rotation at the end of our intern year PGY-1. An inpatient unit is a unit, the purpose, and function of which is to provide services to a patient or client following that person's admission to a health unit. We noticed how frustrated and anxious off-service residents, medical students, and sub-interns were regarding the uncertain expectations, management, and patient rounds. In this article, we will address off-service residents, medical students, and sub-interns as doctors in training. Quality improvement (QI) has become a very vital topic in healthcare and medical education since many medical institutions and hospitals have highlighted the prevalence of suboptimal quality of care in the US health system. Enhanced QI training of the physician workforce has the potential to reduce errors and improve health outcomes. Psychiatrists manage ambiguity in diagnosis as well as the management of patients with psychiatric disorders. The field of psychiatry is very different from any other in the medical field as there aren’t objective findings such as imagining and laboratory workup that could aid in making the correct diagnosis. Psychiatry diagnoses are made by excluding organic causes. Hence, navigating the field of psychiatry can be challenging for all medical professionals. As a teaching program, we have experienced a less than smooth transition of care between the outgoing and incoming teams practicing in the inpatient behavioral health unit. During the beginning of the rotation, medical professionals require ramp-up time to learn how to practice patient-centered and comprehensive psychiatry. Our current approach is “learn by practice”. We believe that with a brief introduction and orientation to inpatient psychiatry we will see a more efficient and confident team early on in their respective rotations which ultimately will improve patient care. In this quality improvement project, we are proposing a PowerPoint presentation for incoming residents and medical students entering the world of psychiatry by rotating through the 5th floor which is the behavioral unit at Larkin Community Hospital. We will have subjects take a survey prior to and after using the presentation tool to assess their knowledge and comfort while practicing in the inpatient behavioral health unit. We will assess the results and quantify the data with visuals to demonstrate the objectives of our quality improvement project. The results of the QI showed how residents and medical students felt more confident, and calm after the PowerPoint guide was provided to them. There was an 80% improvement in confidence and feeling informed among students and residents vs 47 % before the intervention (PowerPoint) was provided. This showed an improvement in the confidence of residents and medical students which translated into better management of patients in the unit. One important gap in the literature is an understanding of off-service residents, sub-interns, and medical students who will be rotating with the psychiatry behavioral unit, which is also known as the inpatient unit. We, therefore, decided to perform a survey of the above-mentioned population to interpret the experience and/or expectations of their upcoming rotation in the psychiatry inpatient unit. Lack of confidence, anxiety, and uncertainty regarding the world of psychiatry can affect patient care significantly. In the psychiatry unit, we have experienced a less than smooth transition of care between the outgoing and incoming teams practicing on the inpatient behavioral health unit at LCH's south Miami campus. During the beginning of the rotation, medical professionals require ramp-up time to learn how to practice patient-centered and comprehensive psychiatry. Our aim was to assist residents, medical students, and sub-interns with the necessary information to navigate effectively in the psychiatry unit by providing a brief PowerPoint presentation that they can review before their first day of the rotation. Subjects were given a survey prior to and after using the presentation tool to assess their knowledge and comfort before practicing in the inpatient behavioral health unit.
Background:
As a teaching program, we have experienced a less than smooth transition of care between the outgoing and incoming teams practicing in the inpatient behavioral health unit. During the beginning of the rotation, medical professionals require ramp-up time to learn how to practice patient-centered and comprehensive psychiatry. It has been well documented in literature how the course of treatment in mental health care is largely affected by the organization of the inpatient team. In fact, therapeutic alliance, confidence, and time efficiency have become an integral part of quality healthcare. This project aimed to improve confidence and facilitate the transition of care and readiness of interns, off-service residents, sub-interns, and medical students by implementing a teaching and reference tool (“Inpatient Guide 101”) which will help us achieve a smooth transition of care by improving knowledge, readiness, and confidence between the outgoing and incoming teams practicing on the inpatient behavioral health unit at LCH's south Miami campus. Unfortunately, there is no existing evidence in the literature regarding this specific problem, which is a strength of the quality improvement project since there is no research available on this matter. There is no evidence that other people have tried to solve this specific problem in the past. No evidence is available regarding what works and what doesn’t to solve the problem. Achieving an easy transition of care of patients between the previous team and the incoming team, reducing confusion and uncertainty amongst professionals. In addition to reducing waiting, the extra processing time is the objective of this project.
Methods:
1. Study Design:
In the months of April 2022 and May 2020, we conducted an anonymous survey of off-service residents, new sub-interns, and medical students who were starting their in-patient psychiatry rotation. Participants were identified with the help of the medical student coordinator at Larkin Community hospital. From the medical student coordinator, we obtained the email addresses of third-year residents. We contacted all the participants (n=30) via an introductory email, including a pre-intervention survey and the intervention. We emailed the survey to all participants via Jotform. We sent an original participation request plus 2 reminders. Respondents received a thank you email after responding to the survey.
1. Questionnaire Development:
The questionnaire was designed using the Jotform survey website. To determine questionnaire domains, we conducted key informant interviews with 2 psychiatry residents who have rotated through the inpatient unit during their first and second years of residency. Owing to the fact that Larkin psychiatry residency or student orientation does not provide education on what to expect in the inpatient unit, we thought previous residents could provide insight into important content and barriers to implementing an “Inpatient Guide”. Domains included Inpatient teams, perceived effectiveness, reported issues with submitting orders, emphasis on attending rounds, sign-out/hand-off instructions, chart review, and various kinds of notes such as discharge summary, quick notes, LAI notes, and direct transfers. To ensure the preciseness of the guide, we revised this “Inpatient Guide” with the psychiatry department's program director. We also conducted 3 revisions with current residents who have rotated through the psychiatry inpatient unit to ensure an understanding of each item in the guide. The pre-intervention survey consisted of 7 items using yes/no responses, likert scales, multiple-answer checklists, and open-ended comment boxes. Residents/sub-interns and medical students were asked about the surveyors’ titles, their knowledge about inpatient workflow, their expectations, and the way they would like to be informed about the inpatient workflow. Open-ended questions asked for inpatient workflow, factors that contributed to hindrances in optimal performance, and suggestions for improving the Inpatient rotation experience. Similarly, the post-intervention survey consisted of 4 items using yes/no responses, Likert scales, and multiple choice answers. This questionnaire was given to the same group of individuals who completed the pre-questionnaire, and was educated by the PowerPoint presentation of “Inpatient Guide 101”. The surveyors received this questionnaire after completing half of their rotation in order to assess the effectiveness of the intervention. 1. Intervention (Educational material) Development Below is a representation of educational material the doctors in training were provided in order to inform and educate them about the LCH psychiatric inpatient unit.
1. Data Analysis:
We received 20 responses from Pre-intervention and post-intervention surveys which accounted for residents/sub-interns/medical students clustered within the same program. Three authors performed a modified content analysis of close-ended responses such as one-word answers, or multiple choice using an iterative, inductive approach to develop consensus on themes and comparisons.
Results: 1.
Sample From our randomly selected sample of 20 psychiatric residents/students rotating in the Inpatient rotation, of which 27% were off-service residents, 20% percent were sub-interns, and 53% percent were medical students. According to our small-scale survey, we were able to find out that 67% of this population was rotating in a psychiatry inpatient unit for the first time, and 33% of this population have rotated in some kind of psychiatry inpatient unit previously. Of that 33% who have already rotated someone prior to this rotation, 60% have rotated elsewhere at least for two rotations, with 40% rotating elsewhere just one time. This allows us to provide vital information to those who have never rotated in an inpatient psychiatric facility (67%) before and ease their apprehensions.
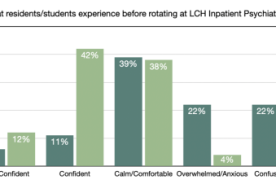
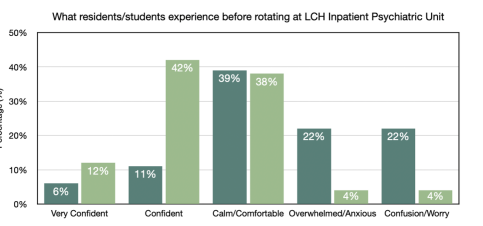
1. Resident/Student Perceptions of Inpatient Workflow Surveyors were asked to describe the feelings they experience on Day 1 of psychiatry inpatient. Content analysis revealed various categories of experiences from very confident, confident, calm/comfortable, and overwhelmed/anxious to confusion/worry. As shown in Table 1, many residents and medical students reported their perceptions about the inpatient workflow prior to starting the rotation. The majority were calm/comfortable, but some felt overwhelmed/anxious (22%) and confused/worried (22%). That is nearly 50% of surveyors who reported a feeling of anxiousness, unreadiness, or being overwhelmed. Data shows that post-intervention, the percentages of both categories dropped to 4%. Furthermore, we saw a significant increase in resident/students’ confidence when we compare pre- and post-intervention surveys. As you can see in the chart below, the surveyors reported 11% how confident they feel pre-intervention, versus 42% post-intervention.
Discussion:
This is the first quality improvement project which is assessing psychiatry residency programs' inpatient
experience or expectations. Being in the unit for an individual who has not had any prior exposure can be
daunting, fearful, and overwhelming. Our survey showed that 67% of this population were rotating in a
psychiatry inpatient unit for the first time, and 33% of this population have rotated in some kind of
psychiatry inpatient unit previously. Unexpected situations can not be planned for, but the new residents,
medical students, and sub-interns should be informed about expected situations and general information
prior to starting. We aim to inform this population by providing accurate instructions that can help them in
their rotation right from the start.
When asked how they feel about starting their inpatient psychiatric rotation, the majority (39%) reported
feeling calm/comfortable, with 11% feeling confident, and 6% feeling very confident. The rest (44%) felt
either overwhelmed (11%), anxious (11%) confused (11%), and worried (11%).
In the survey, we asked a very important question to gauge this population's baseline knowledge of the
psychiatric inpatient unit. Having some knowledge and being informed can decrease anxiety about going
into unknown territory. It allows residents/medical students/sub interns to feel more confident and
hopefully less anxious. We asked about how informed they are about the workflow in the unit. As we
expected, none (0%) reported feeling very informed, 47% stated they were briefly informed, 33% were
somewhat informed and 20% of this population reported not being informed at all. This goes to show how
important it is to give all off-service residents, sub-interns, and medical students a brief informative
introduction to the inpatient unit.
Additionally, we are curious to know which aspect of the inpatient unit were these doctors in training least
aware of. The answer to this question is of utmost importance since we can ensure to incorporate those
aspects into our education (intervention) efforts. The majority were unaware of what inpatient Team A or
B is (41%), and how to write complete patient notes (27%). Other surveyors conveyed their unawareness
or lack of knowledge about how to place orders in Larkins’ EMR called Medhost (20%), and their
apprehensions about rounding with attendings (13%). Next survey we perform, we will improve the
survey by also giving surveyors a blank space to write other areas they want to learn more about, or are
unaware of.
There are many ways to educate this population about the inpatient unit. With our QI project, we wanted
to see which method is preferred the most. It is our intention to use at least two of these methods to
provide all the necessary information to these doctors in training, but we wanted to know their top
preferences as well. The options were to have an orientation by a senior resident, a PowerPoint
presentation prior to starting date, or a one-hour Q & A (question and answer) session with a senior
resident on day 1. The most preferred option for educating these doctors in training about the psychiatric
inpatient unit was to have a senior (post-graduate year 2, 3, or 4) psychiatry resident provide the
orientation, which was selected by 45% of the surveyors. The second preference was to have a
Powerpoint presentation which would be emailed prior to starting with important information about the
inpatient workflow details. In addition to offering convenience to everyone, this option makes it possible
for doctors in training to gain access to this information (PowerPoint presentation) at any time.
They shared their thoughts about how they would feel more comfortable if they had a way to have their
questions answered about the inpatient unit. Over 65% reported that they are going to be rotating in the
inpatient unit for the first time. Whether having a guide may not have monetary gain, or improve patient
safety, as a residency program at a teaching hospital it is our responsibility to keep residents
well-informed so they can perform at optimal levels without feeling overwhelmed or anxious. 41 % of
residents and students reported feeling more oriented on day 1 of their rotation if they received education
prior to starting. Another 24% reported that it will lower their anxiety about the unknown. Although as
residents and students, you want to prepare your best for psychiatry attendings, it is also important to
allow your seniors to perform their duties without being a hindrance. Hence, 18% reported that receiving
education before day 1 will save their seniors (PGY 2, 3, or 4) time from answering repetitive questions,
and allow them more time to see their patients. The rest of the surveyors (18%) said having this
intervention will allow them more time with patients and to complete their notes.
It is interesting to compare our findings with the post-intervention survey. A relatively high percentage of
residents and students are lacking a general understanding of inpatient unit workflow. Notably, residents
overwhelmingly reported positive perceptions about the emphasis on having an Inpatient guide prior to
starting their one-month rotation. In a way, this QI project is about providing a small orientation course
geared specifically towards new off-service residents, sub-interns, and medical students rotating in the
inpatient unit for the first time.
Our findings reveal that there are areas in educating inpatient workflow to residents/students that still
need improvement, including developing and improving inpatient guide 101 on a yearly basis for the
information to be maintained up to date.. Sending this guide every month via email, a week before the
start of their rotation will allow residents/students to feel more informed, and better prepared to work in
the inpatient psychiatry unit. Over 70% of residents reported that the intervention was well organized and
met their needs.
Lessons and limitations:
The lessons learned from this project was learning how important it is to guide our doctors in training for
not just this difficult/challenging rotation but to allow that sense of awareness of other rotations too.
These individuals should have the resources and more for them to perform at optimal levels as residents.
There are many limitations to this project, one of them being the sample size. Since about 15 students
and 2 off-service residents rotate at a given time, it is difficult to increase the sample size. We can combat
that by performing more surveys for an additional 3-6 months to really gauge the situation more clearly.
This project does have generalizability when it comes to applying this type of QI topic to other residency
programs. Since psychiatry residents also rotate in conjunction with other programs such as family
medicine and internal medicine at Larkin Community Hospitals South Miami and Palm Springs
campuses.
Conclusion:
This QI project was designed to provide an inpatient guide for Larkin community hospitals’ doctors in
training who rotate in a short but intense inpatient psychiatric rotation. In essence, it is about providing a
small orientation course geared specifically towards new off-service residents, sub-interns, and medical
students rotating in the inpatient psychiatry unit for the first time. Lack of confidence, anxiety, and
uncertainty regarding the world of psychiatry can affect patient care significantly. We achieved our project
aim by educating and addressing their concerns about the inpatient psychiatric unit. This “Inpatient
Guide 101” will help us achieve a smooth transition of care between the outgoing and incoming teams
practicing on the inpatient behavioral health unit at LCH's south Miami campus. Our intervention did not
add any monetary savings or cost-effectiveness, but it provided clarity, knowledge, confidence, and
comfort for residents and students which will allow them to perform at their optimal level. As a result,
they were less apprehensive and more confident about entering a new environment. The measures we
used in this intervention were appropriate as they provided a clear discrepancy between the preparedness
and mental state of the individual participating in the survey prior to and after using the “Inpatient Guide
101” resource. This QI project is sustainable, and the senior residents will ensure that the intervention
continues with other residents and students who rotated through the inpatient psychiatry unit by
continuing to send this guide every month via email, a week before the start of their rotation will allow
residents/students to feel more informed, and better prepared to work in the inpatient psychiatry unit. The
intervention can be easily modified on a month-to-month basis. As mentioned earlier, this quality
improvement project can and should be replicated in other departments at Larkin Community Hospital,
since residents from one department usually rotate at other departments’ units. The inpatient psychiatry
guide to the psychiatry unit can be easily distributed among different services. Residents and students can
benefit from this type of QI project, which is low-cost, but effective because it saves time, improves
confidence, and clears any apprehensions.
We believe the aim of the project was obtained by educating and addressing medical students, and
residents' questions and concerns about the inpatient psychiatric unit as indicated by the pre and
post-intervention survey. The survey showed an improvement in confidence rating before versus after the
inpatient psychiatry guide to the 5th floor was distributed. We believe that providing the necessary
information about what the expectations of the unit were, improved confidence, readiness, and
collaboration amongst off-service interns, sub-interns, and medical students at LCH.
Our next steps are to widely implement and distribute this inpatient psychiatry guide to all the
departments that rotate through psychiatry at Larkin Community Hospital (LCH) by making this guide
available to coordinations, chief residents, and student liaisons at Larkin Community Hospital. Further
research needs to be done regarding whether or not improving confidence, knowledge, and readiness
among medical professionals can reduce patient length of stay.